Overview
Our work in exploratory and phase I, II & III pharmaceutical trials focuses on the automation and quantification of manual scoring and measurement systems currently used in musculoskeletal clinical studies to reduce timescales and cohort sizes by up to half.
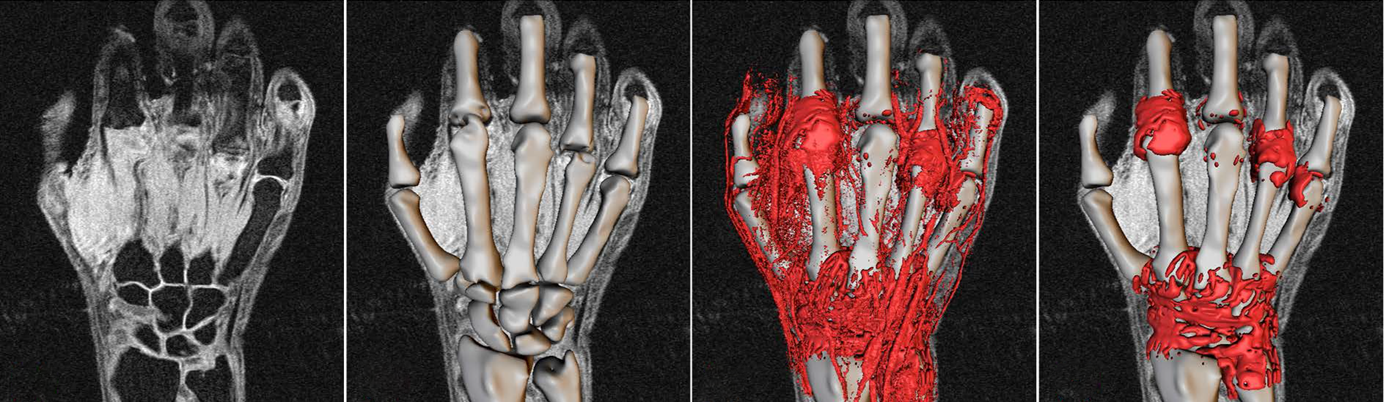
CROs and pharmaceutical companies use Imorphics machine learning algorithms to automatically identify bony and soft tissue anatomy in 3D from MR or CT images, and are able to generate measurements that are highly reproducible compared to the semi-quantitative image reading that relies on human interpretation. The improved sensitivity of these measures can halve the numbers of patients needed to show a clinical effect.
In contrast to categorical scoring systems, continuous quantitative measures of distance, area or volume allow for the use of more powerful statistical methods. Automation means that analysis can be scaled up to large data sets of images with a rapid turnaround time, enabling data-based critical decision points in both retrospective and prospective clinical trials.
In addition to our work on automated scoring methods, we have produced completely novel 3D imaging biomarkers that have demonstrated superior responsiveness to the standard measures. These biomarkers are based on two important principles of our machine learning approach: a complete numerical description of anatomical shape; and the production of thousands of true corresponding landmark points on each of these shapes. This enables the completely objective comparison of 3D anatomy between time points or patients, uncovering exciting and important new insights into disease progression.
Want to know more? Contact us now to talk about how we can help.
Rheumatoid Arthritis
Osteoarthritis